Вызывает ли высокий уровень холестерина болезни сердца и атеросклероз? Вам нужно избегать масла, а как насчет насыщенных жиров? Все о холестерине в этой статье. Также порядок Руководство по холестерину биохакера!
ВВЕДЕНИЕ
Холестерин, вероятно, является одним из самых противоречивых, если не самых спорных тем, связанных с питанием, лекарствами и общим благополучием. Препараты, снижающие холестерин, используются больше, чем когда-либо, яйца все еще избегают из-за холестерина, который они содержат, а высокий уровень холестерина со временем стал вредным фактором. К счастью, эта интерпретация была оспорена в последнее десятилетие, и более обширные данные исследований о холестерине, касающемся наследственности, стали более заметными. Холестерин в яйцах или других продуктах не является вредным, насыщенным «твердым жиром» не забивает артерии, искусственное снижение холестерина с помощью лекарств не всегда может быть хорошим, и побочные эффекты препаратов холестерина также стали лучше понимать.
Холестерин
Холестерин представляет собой структурно стероидный спирт (стерол). Тело способно производить холестерин независимо во всех тканях; Тем не менее, он преимущественно продуцируется в печени. Холестерин также естественно встречается в продуктах питания на основе животных. Холестерин образует жизненно важную часть клеточной мембраны, где он поддерживает как структурный баланс, так и эластичность (около 30% всей клеточной мембраны). В отличие от растений, клетки животных могут функционировать без клеточных стенок благодаря холестерину. Холестерин необходим для биосинтеза стероидных гормонов, выработки желчной кислоты и синтеза витамина D.
Индивидуальный синтезирует приблизительно 1000 мг холестерина в день. В организме хранится приблизительно 35 г холестерина. Взрослые финские мужчины получают в среднем 296 мг холестерина в день от еды; Для взрослых женщин это 210 мг в деньПолем В США среднее потребление холестерина в рационе составляло 293 мг/день (348 мг/день для мужчин и 242 мг/день для женщин) на основе цикла опроса 2013–2014. Ранее рекомендации по питанию для американцев рекомендовали, чтобы потребление холестерина было ограничено не более 300 миллиграммами в день. DGAC 2015 года (Консультативный комитет по диетическим руководствам) не выдвигает эту рекомендацию, поскольку доступна Данные не показывают заметной связи между потреблением диетического холестерина и сывороточным холестерином, что согласуется с выводами отчета AHA/ACCПолем Холестерин не является питательным веществом, представляющим озабоченность из -за чрезмерного потребления. Это связано со значительным генетическим изменением поглощения холестерина и, следовательно, результирующими изменениями уровней холестерина в крови.
Самая богатая холестерином пищей-яйцо. Многие люди продолжают избегать частого потребления яиц, Несмотря на то, что связь с повышенным риском заболевания коронарной артерии и сердечной смертности был опровергнут во всех недавних Исследования и МетаанализПолем Исследования провели не обнаружили сильной корреляции между потреблением яиц и повышением уровня холестерина.
Высокий холестерин и атеросклероз: есть причинно -следственная связь?
Повышенный уровень холестерина сама по себе не является проблемой; Тем не менее, физиологические проблемы возникают чаще, когда повышенный уровень холестерина объединяется с повышенным тихим воспалением, резистентностью к инсулину и повреждением эндотелия, а также с большим количеством частиц липопротеина низкой плотности (ЛПНП) (NB! Не холестерин ЛПН). Ссылка также была найдена между этим и Метаболический синдром.
Повышенные уровни холестерина, вызванные воспалением и эндотелиальным повреждением внутренней стенки кровеносных сосудов, могут привести к наращиванию частиц ЛПНП в кровеносных сосудах (гликопротеиновые сети) и ухудшить приток крови к сердцу, мозгу и другим органам. Исследования показали, что состояние атеросклероза (наращивание бляшки в артериях) Действительно является задержкой субендотелиальных липопротеиновПолем На простом английском языке это относится к строительству липопротеинов на участках воспаления и утолщении стен кровеносных сосудов, тем самым уменьшая просвет (пространство) внутри кровеносного сосуда. Противовоспалительная диета может помочь предотвратить это изменение.
С другой стороны, были предложены теории, что позволяет предположить, что частицы ЛПНП сами по себе являются вредными «посторонними объектами», которые, придерживаясь паутины гликопротеина артерии, вызывают воспаление. Ситуация становится реальной проблемой только тогда, когда воспалительная реакция становится длительной и хронической - создание атеросклеротической бляшки, которая, в свою очередь, образует кристаллы холестерина.
На повреждение эндотелия и воспаление могут повлиять несколько факторов, таких как:
- Хронические инфекции, такой как H. pylori и Chlamydia pneumoniae
-
Микробный баланс кишечника и/или ненормальный
проницаемость кишечника (вызывает эндотоксемию) - Метаболические расстройства
- Экологические токсины (особенно тяжелые металлы)
- Гипотиреоз
-
Генетические факторы
Семейная гиперхолестеринемия
Семейная (генетическая) гиперхолестеринемия (FH) или высокий уровень холестерина должен лечиться для снижения риска сердечно -сосудистых заболеваний. Это обычно делается с лекарствами, хотя диетическое лечение и лечение образа жизни также может быть полезным.
Последний (2017) всеобъемлющий международный мета-анализ показал, что семейная гиперхолестеринемия происходит у 1 из 250 человекПолем Например, в Финляндии частота составляет 1 на 500, хотя наиболее Недавний всеобъемлющий финский обзор (2015) предполагает, что FH недостаточно диагностирован в Финляндии. Распространенность США вероятного/определенного FH оценивалась как 0,40% или 1 в 250Полем Это говорит о том, что 834 500 взрослых США имеют семейную гиперхолестеринемию.
Семейная гиперхолестеринемия возникает в форме гетерозиготы или гомозиготы. Первое значительно более распространено - это означает, что индивид унаследовал неисправный ген только от одного родителя, в то время как другой аллель обычно функционирует. FH включает в себя мутацию в ген-кодировании рецептора ЛПНП или ген кодирующего аполипопротеина-B (APOB)Полем Также были найдены некоторые другие мутации, но они чрезвычайно редки.
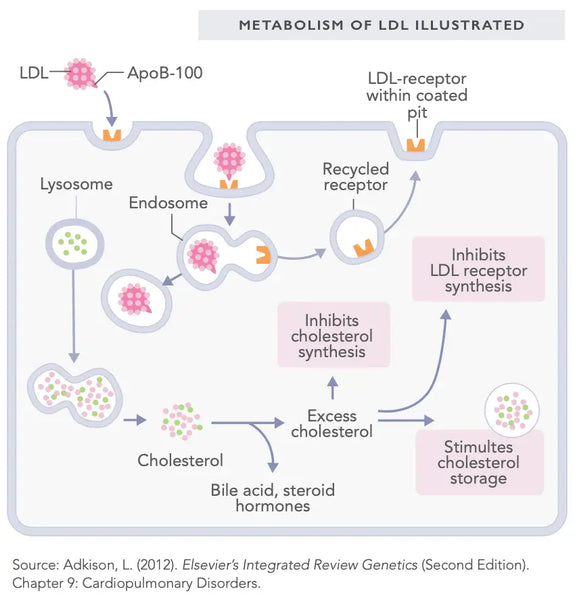
Рецептор ЛПНП расположен на клеточной мембране, где к нему прикрепляются частицы ЛПНП. И наоборот, APOB является частью частицы ЛПНП, которая связывается с рецептором ЛПНП. Аналогия блокировки и ключа может помочь понять их отношения: APOB является ключом, а рецептор ЛПНП - это замок - оба должны хорошо работать для холестерина ЛПНП для транспортировки частиц ЛПНП в клетки и из кровообращения. Когда это разорвано, количество частиц ЛПНП в крови значительно увеличивается. Холестерин ЛПНП, несущий частицы, обычно также увеличивается, хотя они не являются прямо пропорциональными.
Черт! Семейной гиперхолестеринемии диагностирована комбинация клинической картины и лабораторных тестов. Интерпретация всегда требует опыта врача. Как правило, общий холестерин составляет 10 ммоль/л (с диапазоном 8–15 ммоль/л).
Общий холестерин (TC)
Факторы, которые увеличивают общий холестерин, включают Курение, чрезмерное и постоянное употребление алкоголя, необработанный гипотиреоз, диабет, ожирение, менопауза, низкий уровень физической активности и генетические факторы. Диеты с высоким содержанием жиров (такие как кетогенные или низкоуглеводные диеты) также могут временно повысить общий уровень холестерина; однако, Эффект обычно временныйПолем Гипотиреоз всегда следует исключать, если общий уровень холестерина значительно повышен.
Низкий общий холестерин может вызвать дефицит витамина D, проблемы с выработкой стероидных гормонов, депрессия и повышенный риск преждевременной смерти от различных причин.
Гормоны щитовидной железы стимулируют выработку рецепторов ЛПНП в печени. Связывающий половой гормон глобулин (SHBG, см. Раздел 4) связывает холестерин ЛПНП, тем самым снижая уровни холестерина ЛПНП в крови. С гипотиреозом количество произведенных рецепторов ЛПНП недостаточно, оставляя больше холестерина ЛПНП в крови. Это повышает уровень холестерина ЛПНП, а также общий холестерин.
На активность рецептора ЛПНП также влияет инсулин, эффект которого переносится PCSK9. PCSK9 связывается с аполипопротеином B100 на поверхности частиц ЛПНП, что предотвращает их связывание с рецепторами ЛПНП, тем самым блокируя их проникновение в клетки. Чем лучше и стабильнее регуляция секреции инсулина и чувствительности к инсулину, тем лучше функциональность метаболизма холестерина посредством ингибирования PCSK9.
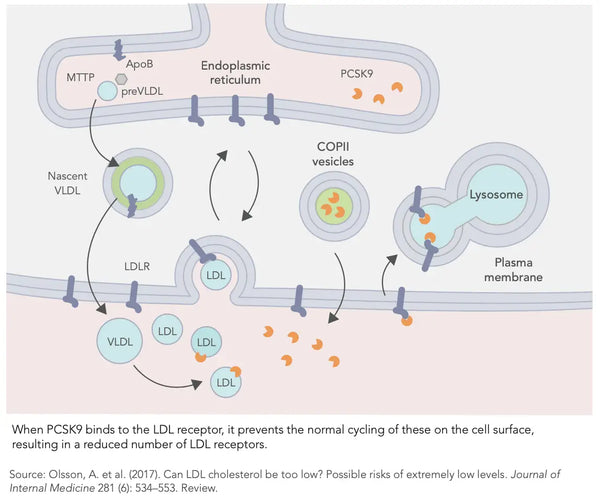
Другим фактором, регулирующим возникновение PCSK9, является воспаление - Чем тяжелее воспаление, тем выше уровень PCSK9, что, в свою очередь, значительно увеличивает уровень холестерина в кровиПолем Наоборот, Более низкий уровень PCSK9 связан с уменьшением воспаления. Высокие уровни PCSK9 также связаны с созданием атеросклеротической налеты (связано с болезнью коронарной артерии).
В 2004 году, Проект северного эталонного интервала (NORIP) Определил эталонный диапазон общего холестерина для здоровых взрослых:
Справочный диапазон для взрослых в соответствии с исследованием NORIP:
- В возрасте 18–29: 2,9–6,1 ммоль/л или 112–236 мг/дл
- В возрасте 30–49: 3,3–6,9 ммоль/л или 128–267 мг/дл
-
В возрасте 50 лет: 3,9–7,8 ммоль/л или 151–302 мг/дл
Аналогичным образом, обследование населения почти половины миллионов человек, в том числе южнокорейские мужчины (30–65 лет), опубликовано в 2000 году, обнаружил, что самая низкая смертность была, когда общий холестерин составлял 5,5–6,5 ммоль/л. (или От 211 до 251 мг/дл)Полем Аналогичный вывод был сделан в последующем исследовании, опубликованном в 2019 году, включая 12,8 миллиона взрослых. Кроме того, Было обнаружено, что слишком низкий уровень холестерина был связан с более высокой общей смертностью по сравнению со слишком высоким уровнем холестерина.
Исследование, проведенное пожилым людям, которые были помещены в больницу, показали, что самый высокий уровень смертности участвовал в людях с самым низким уровнем холестерина (менее 4,14 ммоль/л). Была обнаружена обратная пропорциональная связь между смертностью и уровнями холестерина - Чем ниже уровни, тем выше смертностьПолем Шведское исследование, опубликованное в 1997 году, показывает, что Низкий общий уровень холестерина (менее 4,7 ммоль/л) связан с более высокой частотой депрессии у женщин среднего возраста.
Черт! Эта статья не занимает позицию по использованию лекарств от холестерина. Использование или вывод лекарств следует обсуждать с вашим основным врачом.
P.S. В следующей статье мы обсудим уровень холестерина ЛПВП и ЛПНП, а также то, как вы можете оптимизировать уровень холестерина с помощью своего образа жизни.